 German (DE)
German (DE)  English (US)
English (US)  Spanish (ES)
Spanish (ES)  French (FR)
French (FR)  Hindi (IN)
Hindi (IN)  Italian (IT)
Italian (IT)  Russian (RU)
Russian (RU) When Tamara Taitt moved to Georgia in 2023 to run the Atlanta Birth Center, she found herself in what she calls “an extraordinary position”. Under Georgia law, the center’s own executive director cannot provide routine clinical care for the center’s own clients. She could even face criminal charges for doing so.
Taitt is a nationally accredited midwife. She directs one of the only freestanding birth centers in the state – a destination for women seeking to give birth outside a hospital, cared for by midwives rather than obstetricians. Families choose birth centers to access more holistic, less medicalized prenatal care and birth, and to avoid invasive medical interventions in a state where C-sections occur at three times the rate recommended by the World Health Organization.
But in Georgia, not all midwives can provide that care.
Taitt previously ran another birth center in Miami. She is a certified professional midwife (CPM), with a credential that requires extensive clinical training and allows licensees to practice midwifery in 39 states. But in Georgia, midwifery laws are among the strictest in the country. Only “certified nurse-midwives” – who are licensed nurses in addition to midwives – are licensed to practice there, leaving other trained midwives, including certified professional midwives and traditional community midwives, without a legal pathway.

Even though Georgia suffers from a catastrophic dearth of maternal health providers, Taitt, and other midwives in her position, cannot see clients for routine prenatal visits, take vital signs or “catch” (deliver) babies. All of those clinical tasks are prohibited under Georgia law, with penalties of up to $1,000 in fines or even imprisonment.
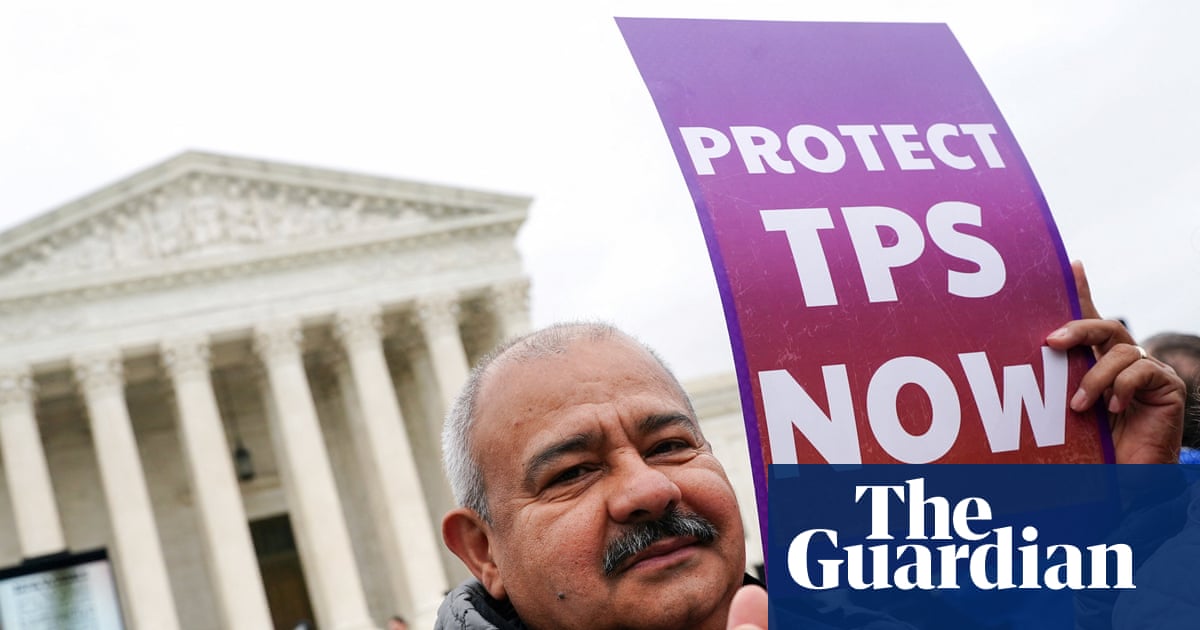
Last week, the Center for Reproductive Rights filed a lawsuit against the state of Georgia on behalf of Taitt and two other midwives challenging those restrictions. The suit seeks to both decriminalize midwives like Taitt, and remove physician oversight requirements for nurse-midwives. The lawsuit follows years of unsuccessful attempts to address midwifery licensing in the state’s legislature.
“I am bringing this lawsuit for every Georgian who has called asking me to be their midwife and who I’ve had to turn down because I could not get a license in this state,” said Jamarah Amani, another plaintiff, at a press conference announcing the lawsuit.

Amani said that the state’s restrictive laws drove her to leave her home state of Georgia. She’s now based in Florida, which licenses a broader range of midwives. Amani works primarily with Black families, including serving young moms and low-income families through a mobile clinic.
Advocates like Angela Aina, executive director of Black Mamas Matter Alliance, see the lawsuit as a critical opportunity for public health intervention in a state where Black women are more than twice as likely to die from childbirth as white women. “In the face of that reality, the state of Georgia is not expanding access to care,” Aina said at the press conference. “It is actively blocking trained, qualified midwives from practicing.”
‘The regulations were about control’
Evidence suggests that midwifery care results in fewer unnecessary medical interventions and better outcomes for both mothers and their babies. But in the US, there is no single standardized pathway to midwifery: certified nurse-midwives, like those who care for clients at hospitals, hold nursing degrees, while “direct-entry” midwives (which includes CPMs and more traditional “lay” or “community” midwives) enter the field more directly, through training and apprenticeship.
Georgia faces a maternal health crisis in which half the state’s counties lack an obstetrics provider, a third of counties qualify as “maternal health deserts” and more than 40 labor and delivery units have shuttered since 1994.
Midwives and lawmakers have long been at odds. A century ago, thousands of traditional midwives served families across the state of Georgia, according to research from Black Mamas Matter Alliance. At the turn of the century, white progressive reformers, deeming midwives “unsanitary and superstitious”, started to push for tighter regulations, physician supervision and burdensome restrictions, including certification requirements, medical bag inspections and literacy requirements.
Federal legislation in 1921, the Sheppard-Towner Act, enacted stricter licensing requirements on midwives across the country, and within two decades, the number of midwives in the state dwindled from 9,000 to just 2,000. “Black midwives are the original maternity care providers in this country,” said Aina. “They sustained entire communities, and they were systematically excluded through regulations that were never about safety. They were about control.”
Sarah Stokely, another plaintiff, lives in Georgia but regularly commutes two hours north to care for mothers in Tennessee. As a certified nurse-midwife, Stokely is licensed to work in Georgia, but found Georgia’s midwifery requirements financially untenable: the state requires nurse-midwives to work under physician oversight, which she said can cost them $1,000 a month. “It’s just not feasible to have a practice here,” Stokely said.

Families in her rural north Georgia community seeking an out-of-hospital birth often drive up to three hours round trip to the Atlanta Birth Center, where they are seen by certified nurse-midwives. Others seek care across state lines. “At the end of the day, it’s Georgia moms who suffer from these laws,” she said.
‘Leaving skilled workers on the sidelines’
Georgia is somewhat of an outlier in the severity of its restrictions, but the legally defined scope of midwives’ practice varies widely from state to state, and some organizations defend restrictions as necessary for patient safety.
In New Mexico, licensed midwives can administer medications and order diagnostic tests independently, while in states like Louisiana, their practice requires physician oversight and is more tightly constrained. Legal battles over who gets to practice midwifery have also played out in places like Hawaii, where the Center for Reproductive Rights challenged restrictions against Indigenous midwives as “medical colonialism”.
Efforts in other states to expand midwives’ licensure and increase their autonomy have prompted pushback from physicians’ groups, citing increased infant risk, the importance of physician oversight and lack of clinical training. Georgia’s current midwifery laws align with the views of the American Medical Association, which has voiced its strong opposition to any legislation expanding nonphysicians’ scope of practice. The American Academy of Pediatrics and the American College of Obstetricians and Gynecology (ACOG) have jointly stated that while they support midwifery-assisted birth, they do not support provision of care by midwives who are not certified by the American Midwifery Certification Board (effectively excluding many lay midwives).
The Guardian reached out to ACOG, as well as Georgia’s nursing board, the Georgia OBGyn Society and the Georgia Hospital Association for comment.
But globally, health organizations like the WHO have urged countries to take steps to expand and invest in midwifery care, suggesting that universal access to such care could prevent more than 60% of maternal and newborn deaths.

And while Georgia’s restrictions criminalize unlicensed midwives administering home births, that hasn’t stopped families from seeking out their care.
Sekesa Berry, a direct-entry “community midwife” who mostly serves Black women, says her clients come to her because they’re afraid of unnecessary medical intervention. “My most common phone call, specifically since the pandemic, is: ‘I don’t want to die,’” Berry said. Those calls often come from first-time mothers who are aware of Georgia’s Black maternal health crisis, or have seen “horror stories” online, and are afraid of experiencing life-threatening invasive procedures in a hospital.
Berry isn’t affiliated with a hospital or birth center – she works for herself and generally administers home births – a traditional way of practicing midwifery that evidence suggests is generally safe for women who have a low risk of complications, are in the care of a qualified midwife and have timely access to a hospital transfer if needed. But most studies on home births focus solely on licensed midwives, and there’s little research on births attended specifically by community or lay midwives who lack certification or licensure.
Despite the law, unlicensed midwives in Georgia have rarely faced criminal charges, although the state’s nursing board has issued cease-and-desist orders demanding that direct-entry midwives stop identifying themselves as midwives. Community midwives say their precarious status makes it harder to coordinate care with hospitals when emergency care is needed.
The state of Georgia has 30 days to respond to the suit. For now, according to Hillary Schneller, the lawsuit’s lead attorney, Georgia remains an outlier: most neighboring states offer some pathway to licensure for direct-entry midwives. Until that changes, Taitt will continue overseeing a birth center that serves mothers she herself cannot clinically care for.
“If not for these restrictions, I could be helping to meet the urgent gaps in maternity care, including for clients at our own birth center,” Taitt said at the press conference. “Instead, Georgia is choosing to leave a skilled, committed workforce on the sidelines even as communities struggle to access care.”




















Comments